A few years ago I had a blog series called ‘Inactivity and Metabolic Health‘. It was an examination of the science of physical activity as treatment for metabolic issues caused by insulin resistance. Exercise improves insulin sensitivity. As far as I’m concerned, that is exercise’s most important effect on the human body. The reason I was interested (and continue to be) in the subject was my own experience – a long history of hormonal and metabolic issues that disappeared when I changed my habit of inactivity and became physically active.
I’ve written about it before, but to review: from my early teens I struggled with a constellation of symptoms that traced back to insulin resistance. Severe cystic acne, weight gain, irregular (and frequently absent) periods, ovarian cysts, fibrocystic breasts, elevated blood pressure as I got older, blood sugar dysregulation and panic attacks, depression, migraines. My doctor told me year after year after year to exercise, and I resisted and resisted. Went so far as to convince myself she was ‘blowing me off’ and just didn’t know what to do. I consulted natural health books and tried things like putting garlic suppositories in my vagina and drinking bentonite clay. Funny thing, those things never worked. I tried fad diet after fad diet, some worked temporarily, but most just made the problems worse.
At 35 (eight years ago), weary from the decades of being battered by the predatory winds of natural health mythology, I decided to finally do what my doctor had been admonishing me to do for so long – start exercising. And the rest is sort of history. It completely changed my life and my health. I lost weight I’d been unable to lose for years. Many of my health issues resolved. My depression and anxiety receded. It was pretty amazing. And flew in the face of the entire diet industry which ties weight and health almost solely to diet, and the fitness industry, which fixates myopically on the aesthetic results of exercise with very little attention to the health benefits (which are much more profound).
As I got more into fitness and began to lift weights, I became aware of the ‘cardio bunny’ meme, and noticed a certain disdain for cardio among the crossfire/strongman/dude bro element of the fitness industry. I read lots of blog posts about how ‘cardio makes you fat’ (hahahahahhhhaaahahhaahahahhhaah, yeah right), and how people who did cardio were all ‘skinny fat’, blah blah blah. If you’ve been around for a while, you are probably aware of the memes I’m talking about.
But I did enjoy cardio, especially the way it made me FEEL, and so I kept doing it even if it meant I would end up the dreaded skinny fat (PS, what the fuck is wrong with being skinny fat? Nothing.)
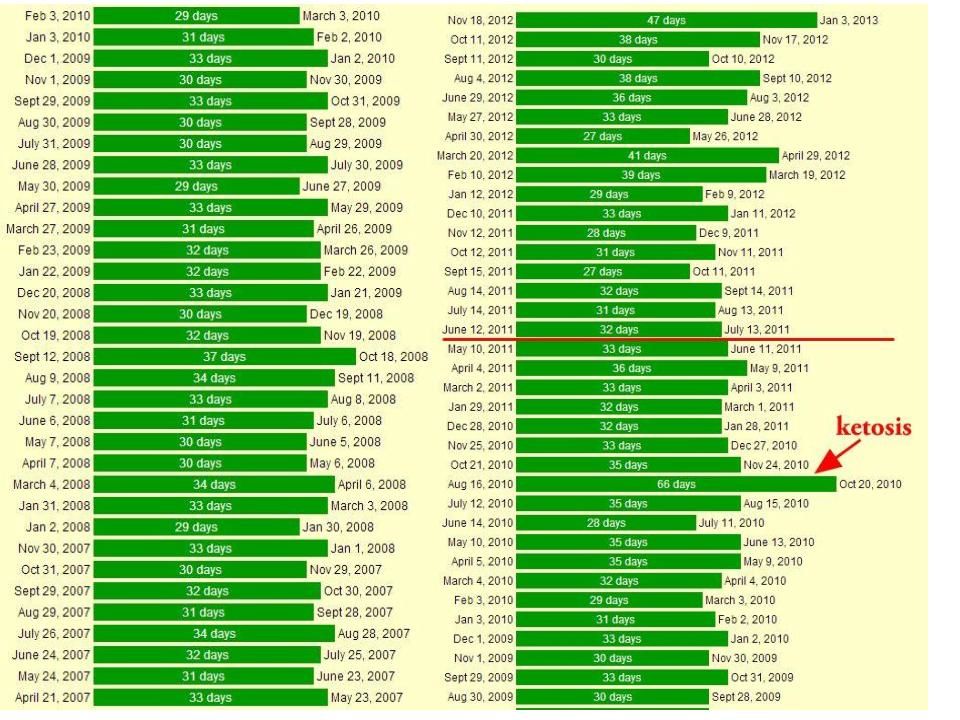
The more cardio I did, however, not only did I not get fat or even skinny fat, in fact I continued to get leaner. And I continued to get healthier. By 2012 I was training for a half ironman. I was doing as much as 4 hours of cardio a couple times a week. Don’t get me wrong, I was lifting too, but not nearly as much as I was doing cardio. I can look back at the time I was training for the half ironman and see that that was the leanest and healthiest I’ve been in my life. I had tons of energy. My depression was non-existence. My blood tests showed I was off-the-charts healthy. My period was like clockwork. And I was maintaining a body fat percentage of like 15% while eating as much as 4000 calories a day. See for yourself:
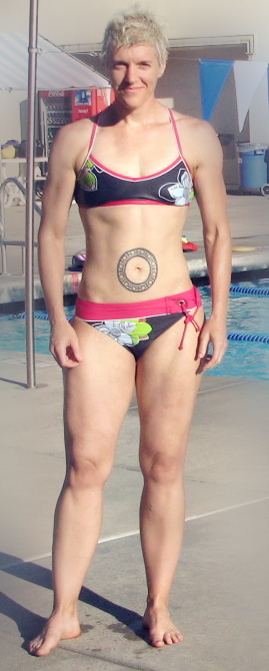
160-ish pounds. Training for a half-ironman. 1-4 hours of exercise a day, 4 days a week, including 2 strength trainign sessions a week. 4000+ calories a day.
I. Felt. Fucking. Awesome. I felt like I could take on the world, and win. I didn’t just feel physically awesome, I felt emotionally awesome. Confident. Strong. Outgoing. Optimistic. It was one of the best times of my life.
And so, I talked a lot on my blog about the benefits of exercise, especially for those with predispositions to insulin resistance (like me). Exercise did for me what no dietary intervention had ever been able to – normalize my blood sugar regulation, improve my insulin sensitivity, allow me to eat anything and my body metabolize it just fine and use it for fuel. Exercise made my body work right. And all of this was supported by decade upon decade of credible peer review research showing exercise – specifically cardio – is a primary intervention for metabolic syndrome and insulin resistance. Exercise improves insulin sensitivity, there is absolutely NO question of this in the scientific literature.
And when my body was working right, it was able to use the food I ate – WHATEVER food I ate – to build muscle and create energy. Energy I used to go out and live an awesome life. Write prolifically. Make huge waves in the fitness industry. Piss off the fad diet gurus ROYALLY.
Ah, but it was fun.
Things started to fall apart a little about a year and a half ago when my knee arthritis got really bad, bad enough to affect my ability to exercise the way I had been. The first thing to go was running. Then cycling. Then I had to cut down the amount of time I was spending on the elliptical, because it would make my knee swell and ache badly. I had surgery 9 months ago in an effort to increase my range of motion and pain levels. That sidelined me completely for a couple months, and then when I got back to exercising, it was more lifting than cardio. I like lifting, don’t get me wrong. And I’m glad I’ve been able to keep doing it! but it’s been a long slog through recovery and trying to get back to the amount and intensity of cardio that was so helpful for me. I’m still not there.
And the result has been that in spite of still lifting, I’ve seen my depression came back. BOY did it come back. I’m still really struggling with it, somedays I can’t even get myself out of the house. Recently my cystic acne has cropped back up. I recently had my first migraine in 6 or 7 years. My HDL is creeping downward. My period is no longer like clockwork. And my weight has crept up in spite of reducing my calorie intake (this is due in large part to some meds I’ve been taking, but I have a gut feeling that my weight gain would have been smaller if I’d been able to keep exercising the way I need to exercise). Creep may be an understatement, I gained 25+ pounds in 2015.
A year without the kind of cardio that my body needs has resulted in a lot of my health issues re-emerging.
FUCK.
Cardio, not lifting, completely turned my life around. And the more cardio I got, the better. My friend Sol (from examine.com) did a guest post here a couple years ago addressing head on the ‘cardio makes you fat’ meme. In short, it’s bullshit. Cardio does not make you fat. And if you’re like me and prone to insulin resistance, it may even make you leaner and healthier than lifting alone. The research certainly bears out the value of cardio for metabolic health. Sure, ‘lifting weights faster’ may work for some young healthy people. Heck, it may work for some older healthy people.
For me? Older and predisposed to insulin resistance? I need the cardio. And lots of it. I get my hour a day of heart pumping cardio and I can eat pretty much anything and take it in stride, and THRIVE. Take away my ability and access to that level of cardio and my health deteriorates.
This is important. KEEP THIS IN MIND next time you start judging ‘lazy people’ for not ‘doing what it takes’ to get the exercise they need to be healthy.
Some people simply don’t have access. You know what I had that allowed me to get 1-4 hours of cardio a day? Lots of spare time. A gym membership. Safe spaces to exercise. Money to spend on equipment. Did I mention time? Lots of free time? Oh, and transportation to and from the gym. And different options at that gym. I can swim, well, because I had years of lessons as a child and access to a pool.
Do you know how many people don’t have any those things I just mentioned, let alone all of them? At times, I fell into thinking ‘if I can do it, anyone can’. But, not everyone can. Many, MANY people can’t, whether it be because they don’t have access to a gym, a safe space to exercise, money for equipment, or the ability to swim (or one of any number of other privileges that makes exercise a luxury).
For many people, exercise isn’t a matter of ‘priorities’. They are not ‘making excuses’. They simply do not have access.
Let me tell you about how things are for me now. I am semi-disabled. There are a lot of physical things I can’t do. Yet, at least. My knee is healing very slowly. And, I am depressed. There are days I can’t make it out of my house. This isn’t a matter of not being motivated. This is a real medical condition. I know that getting more active will help with the depression, but sometimes the depression is so bad it keeps me from being active. And when I CAN be active, I am not strong enough yet to exercise as long and as intensely as I could when things were going so well for me physically.
I have lost several of the privileges I enjoyed 3-4 years ago that gave me the option of getting the exercise I needed to thrive. I will probably get them back – and I still have several other privileges that increase my likelihood of getting them back. I still have the gym membership. I still have transportation. I still have a safe space to exercise. I still have enough money to afford equipment. As my knee (and head) heals, I’ll be able to continue building my activity back up.
But there are many people out there that are far more trapped than I am. Who may not have ANY of the privileges I enjoy. People for whom the fight to be active isn’t currently winnable. Judging those people as lazy and unmotivated isn’t fair. The answer isn’t to judge and ridicule them. It is to create safe spaces. Make facilities accessible. Provide reliable transportation. Provide fair and equal medical treatment (I will be writing about this in the near future). Taking mental illness seriously. No, it’s not laziness or lack of motivation. Depression is REAL, and debilitating. Mental illness deserves compassion and treatment. NOT ridicule. And that’s just the invisible disability. Many people are visibly disabled, and they need access to safe fitness options as well.
Why? Because fitness isn’t about APPEARANCE. It’s about health. It’s about quality of life. It’s about saving our country billions of dollars in medical costs. It’s about guaranteeing everyone the same quality of medical care, fitness accessibility and compassion.
We need to do a couple things.
- Reframe fitness from ‘aesthetics’ to health.
- Improve accessibility. The Y is on the frontline of this massive endeavor, and has been for decades. Look into what your local Y is doing in your community. Volunteer, donate.
- Stop judging and ridiculing people for not exercising (if you do). You don’t know what barriers they may have, and just because YOU have been able to overcome barriers doesn’t mean everyone has the same barriers and abilities to overcome them. Welcome people of all shapes and sizes and colors and ages and abilities to your gym. Fitness can and should be for everyone. Not just the already fit and able.
- Stop spreading the elitist and misguided meme that cardio makes you fat. It can be LIFESAVING for people with insulin resistance. It can also be more accessible than lifting for many people without access to a gym and equipment. And it doesn’t need to be an either/or question either – both are beneficial and it’s perfectly fine to combine them. And EVEN IF CARDIO DID MAKE YOU FAT, there are worse things to be than fat. Like, an elitist asshole.
- Stop, also, spreading the myth that exercise is for aesthetics and isn’t important for health. IT IS VITAL for health. VITAL. An exercising body doesn’t need fad diets. An exercising body can metabolize carbs and fat and protein and use it all for fuel. People with medical conditions may need special diets, but those diets should be prescribed and administered by medical professionals, not diet books and internet gurus. Fad diets serve NO ONE, except the bank account of the fad diet book authors. They are also generally quite elitist, time consuming and rely on expensive, and hard to find foods that most people simply don’t have access to. OR NEED.
Cardio is awesome (especially for people with a predisposition to insulin resistance). Lifting is awesome too. Fad diets SUCK and no one should be using them. People with medical conditions that require dietary intervention need to work with a medical professional to administer that dietary intervention. Fad diets offer false and misleading hope that all our problems can be solved with diet. NOPE. The research suggests that if there is anything close to a magic pill, it is EXERCISE. Not magic diets.
___________________
Got something to say about this post? Join the discussion on Facebook!
I mentioned that it was the habit of inactivity that kept me from improving my health. In order to make long-term changes, I needed to change my habits to support regular and sufficient exercise. I did it by focusing on making one small change at a time, and practicing those changes consistently over time. It worked. It worked so well that it’s the approach I take with my coaching clients. And it’s the foundation of the group coaching program I created with my coaching partner Sean Flanagan (The Habit Project'). We’ll be enrolling our next session of the Habit Project on April 5th. If you’re interested in learning more about this approach to behavior change that we’ve seen work for hundreds of clients over the years, get on our pre-enrollment list here. Only people on the list will be getting the invitation to enroll in the program! Putting your name on the list does NOT obligate you to join the program.